
[Euthanasia in Canada #2] The Canadian Euthanasia Bill: The process from application to completion and safeguards to avoid the risk of coercion
- リップディー(RiP:D)

- Dec 1
- 9 min read
[The process from application to completion, as seen in the Canadian Euthanasia Bill, and safeguards to avoid the risk of coercion]
This paper focuses on the euthanasia law in the Netherlands.
・"The specific process from requesting euthanasia to its completion"
- "Safety measures in place to prevent harm to patients"
--I will explain this while focusing on the above two points.

Official Canadian Government Website: A very easy-to-understand site for the general public

" Euthanasia and Assisted Suicide Review Act " PDF
[Legal name]
Medical assistance in dying: Legislation in Canada
It is commonly referred to as MAID , and is equivalent to what is called "euthanasia" in Japan.
Euthanasia has been legal in Canada since 2015 in Quebec and in the rest of Canada since 2016 .
[Eligibility conditions]
Eligibility for public medical care (meeting requirements for residence and waiting period, etc.)
Are 18 years of age or older and have the capacity to make medical decisions
Voluntary application (no undue external pressure)
Informed consent (consent after receiving information about alternatives, including palliative care)
" Grievous and irremediable medical condition":
‣ Serious and incurable illnesses, diseases, and disabilities
Irreversible decline in abilities (severe decline in physical, social, occupational, or other functions important to the individual)
The condition causes "persistent suffering that is intolerable to the individual and cannot be alleviated by the individual's tolerance."
Points to note when assessing pain
A broad understanding of physical, psychological, social and existential aspects
Consistency between the patient's story and their clinical picture/historical history
Whether the pain is due to a medical condition or decline
Whether the pain is persistent
Respect for subjectivity (pain belongs to the individual's subjective view)
remarks
- Somewhat similar to the Dutch euthanasia model ( also allows for non-terminal illnesses ).
In other words, patients with existential pain due to dementia or cervical spinal cord injury (unable to move below the neck) are also within the acceptable range.
*However, euthanasia for medical conditions where mental illness is the sole underlying condition (MAID MD-SUMC) was scheduled to be legal from March 17, 2024, but unfortunately, due to the widespread global rumors of a Canadian euthanasia conspiracy , this has had to be postponed until March 17, 2027 .
[Review process] (Euthanasia in Canada)
*Points to note in advance
Note the two "Track" terms.
Track 1: ( End stage )
Applications from patients whose natural death is reasonably foreseeable .
Track 2: (non-terminal )
Applications from people whose natural death is not reasonably foreseeable .
→ Additional safeguards (such as a 90-day waiting period or expert consultation) are required.
*MAID is discussed in terms of two types: Track 1 euthanasia and Track 2 euthanasia.
Roughly speaking, it refers to whether the patient is in a "terminal or non-terminal" state at the time of requesting euthanasia .
In Canada , euthanasia for non-terminal illnesses became permissible in 2021, more than five years after the law came into effect.
This is a unique expression of euthanasia in Canada.
For more details, see the previously mentioned article
↓
[ Canadian Euthanasia #1 ] Current Status and Performance Data: Maid (Active Euthanasia/Assisted Suicide)

[Application stage]
(Initial response at the time of application)
1. Expression of intent from the individual :
MAID is based on the individual's wishes and can never be performed at the direction of another person.
2. Initial explanation :
- Explain the MAID system/requirements, alternatives including palliative care , and the freedom to withdraw (at any time).
- (Track 2) Providing information on counselling, mental health and disability support, community services, palliative care, etc., and suggesting referrals to professionals as needed.
3. Prepare a written request :
Signed and dated by the person (or by a scribe, if permitted by law) , and signed and dated by an independent witness present.
4. Confidentiality :
The fact that a MAID has been applied for or provided will not be disclosed without the individual's consent.
* Notes regarding Voluntariness & Informed Consent
Confirm that the application is made voluntarily (without undue influence from family members, medical professionals, etc.).
Consent will be obtained directly from the individual (consent from a proxy decision maker is not permitted).
What to include in your description:
Reasonable and acceptable treatment options (benefits, risks, and side effects) and palliative care
(Track 2) Information on support services (counseling, mental health, disability support, community/income/housing support, etc.) and suggestions for referral to professionals
The possibility of withdrawal at any time (opportunity to withdraw even immediately before implementation)
Possible complications for each method (donor administration/self-administration, possible non-fatal complications, etc.)
If you choose to self-administer :
There is a possibility that the treatment may not work or may persist, and in such cases, the individual's consent must be obtained immediately before the treatment can be switched to administration by another person .
Alternatively, enter into an advance consent for provider-administered MAID.
[Evaluation stage]
Two assessors (mainly physicians) (first: provider + second: another assessor).
Evaluated independently and separately from each other.
Track 1 (natural death is reasonably foreseeable = terminal)
Written requests must be signed and dated in front of an independent witness .
If communication is difficult , reasonable accommodation will be provided to help understand and express one's wishes.
Immediately before implementation : Provide an opportunity to withdraw and obtain explicit final consent (unless there is an exemption listed below).
*Waiver of Final Consent :
Only in Track 1 can a written agreement be made between the individual and the provider regarding the provision of information after the individual loses capacity (the terms and format are subject to the regulations of each jurisdiction).

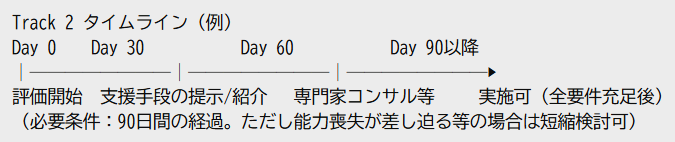
Track 2 (natural death not reasonably foreseeable = non-terminal)
The same was true for two independent reviewers.
Additional requirements:
A minimum period of 90 days (a 90-day "waiting period" from the start of the evaluation).
Provide the individual with information about reasonable and available means to alleviate their suffering (counseling, support services, community services, palliative care, etc.) and suggest referrals .
The provider and assessor will agree and confirm whether the individual has "fully and seriously considered" the measure .
Consultation with a practitioner with expertise in the underlying disease (if neither the provider nor the assessor has expertise in the disease).
90-day reduction : If a provider considers reducing the period due to imminent loss of capacity , etc., an assessor's opinion (whether loss of capacity is imminent) is required.
[Implementation stage]
method
Provider-administered MAID :
A doctor or NP (Nurse Specialist) administers the drug to cause death.
Self-administered MAID :
A doctor/NP prescribes and provides medication, and the patient self-administers it, resulting in death.
When self-administering, the possibility of failure or prolonged administration should be explained in advance.
If advance consent is signed, if self-administration is unsuccessful or prolonged, it is possible to switch to donor administration if certain conditions are met .
Drug safety management
Notification to Pharmacy Office :
When prescribing or receiving medication for MAID purposes, communicate that purpose to the pharmacist .
Safe prescribing, storage and return : Ensure the safe use, storage and return of relevant substances.
[Just before implementation and reporting stage]
・Just before implementation:
Confirm explicit final consent with opportunity to withdraw ( unless a final consent waiver or prior consent for self-administration is in effect in Track 1 ).
·implementation :
Safely administer via the chosen method (donor-administered/self-administered) in accordance with clinical guidelines and site protocols.
Death certificate :
Written in accordance with the rules of each jurisdiction.
・Records and reports :
The medical record will include information such as the evaluation details, consent, explanations, and coordination.
Filed under the federal reporting system and additional state and territory reporting requirements .
*Notes:
・This explanation is based on the standard model .
Depending on the state or territory, there may be differences in formatting, witness requirements, specific procedures for final consent exemptions and prior consent, reporting formats and deadlines, etc. Practice must always follow the rules and guidance of the relevant jurisdiction.
・Doctors have the right to conscientiously refuse to diagnose a patient . (This is a universal rule.)
【remarks】
The process for implementing euthanasia (MAiD) in Canada can be roughly organized as shown in the diagram below.

The decision on whether or not to permit euthanasia will be made by two independent physicians , each from their own professional perspective, in consultation with multiple medical and welfare professionals as necessary.
Some critics have criticized the system for being "lax in its screening process." Such criticisms tend to be based on religious values (see below), and there are also occasional instances of criticism citing the system in the Benelux countries.
However, in the Netherlands, in addition to the first and second reviews by two independent doctors, there is also an administrative organization (regional review committee) that acts as a third check function , and in practice, a more multi-layered review system has been established.

In contrast, Canada (and the United States) does not have a "third-party checking agency" like the Netherlands, so there is a certain degree of rationality in pointing out that the system as a whole has relatively weak protective measures (safeguards).
This background is one of the reasons why the WHO, UN human rights agencies, and others have expressed concerns about the operation of the system.
By the way, in Japan, regarding Canada's assisted dying (MAiD) system,
"The disabled and economically disadvantaged are being forced into euthanasia."
"The application process for euthanasia is easier than that for welfare benefits."
We are seeing the spread of so-called "dystopian conspiracy theories" such as these.
However, we would like to make it clear that these claims are misinformation that is far removed from the facts and are baseless rumors .
Behind this misinformation lies the "strong information dissemination power" of fundamentalist Christian media in North America .
In North America in particular, unlike Japan, there is a structural characteristic in which religious media (Christian conservative media) has a strong influence on political and social discussions .
These media outlets believe that the establishment of euthanasia is a violation of their own
Religious doctrine (view of life and death, taboos)
moral values
Influence (interests) of related organizations
They tend to feel a strong sense of crisis, seeing it as a threat to their country.



An organization that repeatedly files lawsuits (total ban on abortion) based on Christian bioethics
"Euthanasia is suicide and a despicable act that goes against (Christian) bioethics."
"Suicide is a blasphemous and shameful act that betrays God."
"Suffering has meaning, as in the Passion of Christ."
As a result, manipulative opinions are often disseminated that exaggerate facts or generalize certain special cases in order to deny the system (explained in more detail in a separate article).
Much of the misinformation that has entered Japan, such as "Canada has become a society that forces the weak to die," is the result of translations and propagation of these religious fundamentalist messages originating in North America . Of course, there are Christian groups in Japan that are closely related to them (explained in a separate article).
The situation is somewhat similar in Japan as well.
When the introduction of euthanasia is discussed,
Organizational reputation
Existing influence and vested interest structures in the social security field
Consistency with religious group doctrines
There are examples where people who are concerned about factors such as these become the ``source'' of information dissemination.
This is explained in more detail in the section on euthanasia in Japan.
You should also check the following facts:
Canada's assisted dying (MAiD) system has one of the most transparent statistical and reporting systems in the world , with all cases published in annual reports, so if claims such as "death is forced upon the weak" are true, they will certainly be visible in the statistics.
In addition to government statistics, international research companies have also intervened, and the rumors have been denied, with the criticism of Canada already calming down .
Non-terminal cases (Track 2) still account for around 4% of the total (622 people in 2023) , and no evidence has been found that the system is being abused.
It is also important to emphasize that Canada has a provincial system of ethical review and medical supervision , and that a framework has been established to prevent doctors from making arbitrary decisions.
If we are truly concerned about the "forced death" of vulnerable people in Canada, we should rather be concerned about the "forced death" of vulnerable people in Japan.
Cases where applications for welfare benefits were not properly accepted, leading to starvation or suicide due to poverty
Unable to bear the pain of illness, many people resort to suicide by jumping onto trains.
Isn't it necessary to pay closer attention to these "real problems occurring in Japan" ?
Before making excessive claims of crisis about the Canadian system, we should first reconsider the need to address the challenges that are already apparent in our own country .
![[Euthanasia in the United States #2] (From Oregon Law) The Process from Requesting Euthanasia to Ending It: Details of Safeguards to Avoid the Risk of Coercion](https://static.wixstatic.com/media/1e6e15_98f8a8a03daf4c6a923030bbece140d7~mv2.png/v1/fill/w_980,h_551,al_c,q_90,usm_0.66_1.00_0.01,enc_avif,quality_auto/1e6e15_98f8a8a03daf4c6a923030bbece140d7~mv2.png)
![[Euthanasia in Australia #2] The Australian Euthanasia Bill: The process from application to completion and safeguards to avoid the risk of coercion](https://static.wixstatic.com/media/1e6e15_07d9ead448aa41d6b149858bf7988cf6~mv2.png/v1/fill/w_980,h_551,al_c,q_90,usm_0.66_1.00_0.01,enc_avif,quality_auto/1e6e15_07d9ead448aa41d6b149858bf7988cf6~mv2.png)
